CRANIAL NERVES IN REVIEW
 Updated 5/24
Updated 5/24Dear nurses,
Stroke Series Assessment is no longer available.
The largest of the cranial nerves, is the Trigeminal.
This nerve contains three branches:
Opthalmic ( corneal blink reflex).
Maxillary - which supplies the upper jaw
Opthalmic ( corneal blink reflex).
Maxillary - which supplies the upper jaw
Mandibular - controls the lower jaw.
Learn more :Cranial nerves

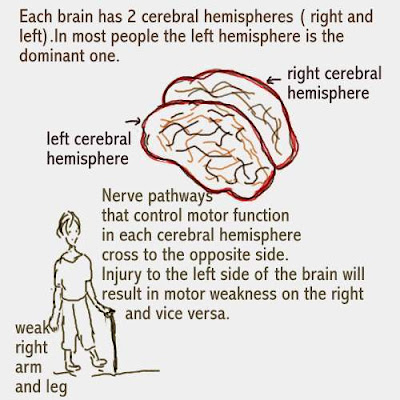
In the image above, Ann is an opera singer.
While on stage, she suddenly starts having
trouble getting her words out. Her right arm
also feels weak. These symptoms are classic
of stroke symptoms.
Severe headache, mental confusion, visual
disturbances and right or left sided weakness
ma occur.

Learn more: The care plan
For more helpful information, please click on the links below:
posted by Margaret at
7:25 PM
|
0 comments
![]()
![]()
.JPG)






































{kind=link}
{kind=link}