WHAT IF YOUR PATIENT IS IN A COMA
Updated 10/25

Dear nurses,
New information has been added below.

Scenario:Henry is a 35 year old male,
who had a traumatic brain injury.He has
been in a coma for two weeks.
who had a traumatic brain injury.He has
been in a coma for two weeks.
His family members do not believe there
is hope.Whenever they visit, they speak
negative things.

negative things.
It is important to remember, that a patient
in a coma can still hear. There are stories,
where patients have repeated all they have heard.
in a coma can still hear. There are stories,
where patients have repeated all they have heard.
Please watch the video: Can a comatose patient hear?

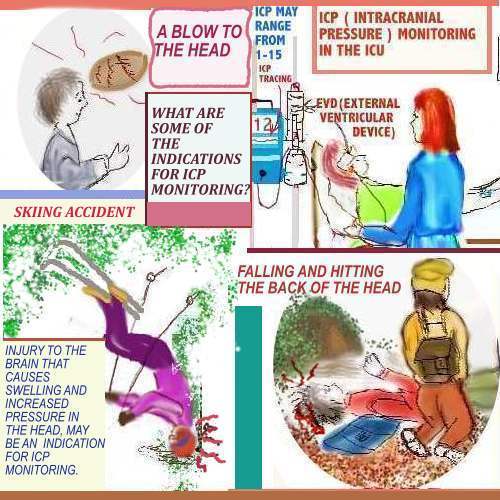
Scenario: Above, is a person who went skiing and
sustained head trauma.This is an indication for
ICP monitoring.There are many other reasons
that ICP monitoring may be necessary.
sustained head trauma.This is an indication for
ICP monitoring.There are many other reasons
that ICP monitoring may be necessary.
Learn more about this topic, by clicking on the
link: ICP monitoring
link: ICP monitoring
posted by Margaret at
7:26 AM
|
0 comments
![]()
![]()




 Dearnurses.net is no longer available.
Dearnurses.net is no longer available.































.JPG)




{kind=link}
{kind=link}
{kind=link}